
Use of RBC indices in identifying thalassemia
RBC indices can be useful in identifying thalassemia, and several indexes have been suggested for discriminating between thalassemia and iron deficiency anemia (IDA).
Differentiating thalassemia from iron deficiency anemia
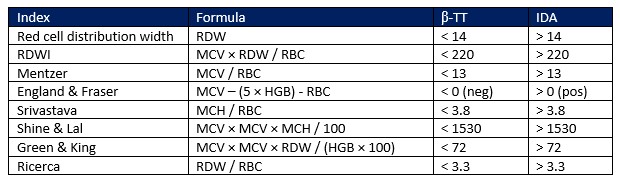
Iron deficiency is the most common cause of anemia and arises when the body’s intake and storage of iron is insufficient to fully support erythrocyte production (1, 2). Thalassemia is another cause of anemia, with 50% of the world’s cases in Southeast Asia (3). In Pakistan, thalassemia is the most common inherited disorder, with an estimated frequency of occurrence of 5%–7% (3, 4). Both iron deficiency anemia (IDA) and thalassemia are manifested as microcytosis and hypochromia, with low hemoglobin concentration as a result. However, while IDA is a nutrient disorder that can be treated with iron supplementation, thalassemia is an inherited disorder that lacks management protocol and for which blood transfusion is a mainstay of treatment (4, 5). The ability to differentiate IDA from thalassemia is important, as blood hemoglobin will not be improved by iron supplementation in thalassemia patients (6). Together with determination of, for example, serum iron levels, RBC indices can be of good help (3, 6). Many formulas that include the RBC indices have been suggested to discriminate thalassemia from IDA (Table 1), of which RDW index (RDWI) followed by Mentzer index have been found to provide the highest rate of correctly diagnosed patients (3, 6).
Cell discrimination method
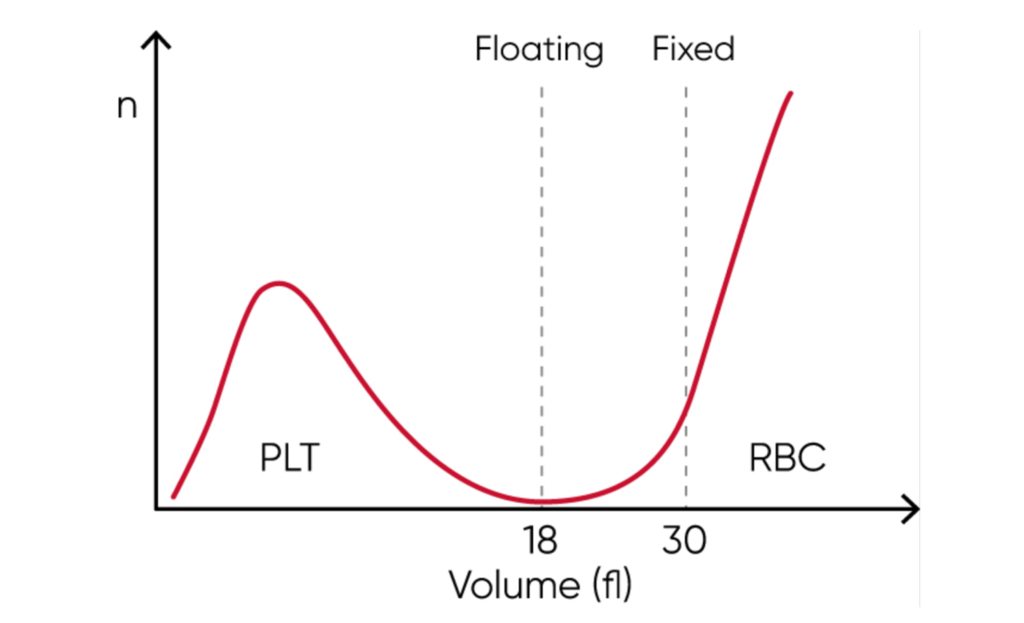
High accuracy in RBC counting and sizing and HGB determination is the foundation for reliable reporting of the RBC indices that constitute the foundation for clinical decisions in anemia investigations. Many legacy cell counters use a fixed discriminator at 30 fL for separation of RBC and PLT populations. However, excessive number of PLTs might interfere with the mean red cell volume (MCV) parameter. Similarly, microcytic RBCs with low MCV can give falsely elevated PLT counts, as the minima between PLT and RBC histograms cannot be identified due to the mix of microcytic RBCs and PLTs well before the cell size discriminator at 30 fL. Such effects can be minimized with floating discriminator technique that estimates the best separation between cell populations. Boule’s 3-part hematology analyzers use a discriminator that floats between 10 and 28 fL, thereby preventing the microcytic RBCs to be falsely counted as PLTs (Fig 1).
Learn more
Read more from the white paper Clinical utility of red blood cell indices in anemia investigations
References
- WHO: Anaemia. who.int/data/nutrition/nlis/info/anaemia (accessed 2023-08-24).
- Miller, J.L. Iron Deficiency Anemia: A Common and Curable Disease. Cold Spring Harb Perspect Med 3, a011866 (2013).
- Niazi et al. Usefulness of red blood cell indices in differentiation of microcytic hypochromic anemias. Gomal J Med Sci 8, 125–129 (2010).
- Khaliq, S. Thalassemia in Pakistan. Hemoglobin 46, 12-14 (2022).
- Li et al. The Efficacy and Safety of Vitamin C for Iron Supplementation in Adult Patients With Iron Deficiency Anemia: A Randomized Clinical Trial. JAMA Netw Open 3, e2023644 (2020).
- Jameel et al. Differentiation of beta thalassemia trait from iron deficiency anemia by hematological indices. Pak J Med Sci 33, 665–669 (2017).